The technology is innovative in its use of MANETs for implementing and tracking behavior therapies. MANETs are of major interest to the defense, homeland security, and disaster preparedness research sectors and are likely to continue to increase in sophistication throughout the foreseeable future. The essential quality of MANETs that make them well-suited for behavior therapies is their ability to support so-called ‘pervasive’ or ‘ubiquitous’ computing. Because the nodes of the network are free to move about in space, the individual will come into (and go out of) contact with various nodes of the network including human and automated sensors. The network is able to reassemble on-the-fly, thereby enabling behavior modification to travel with the individual undergoing therapy. This enables therapy to continue at home and school in a seamless fashion.
The technology is innovative in its use of MANETs for implementing and tracking behavior therapies. MANETs are of major interest to the defense, homeland security, and disaster preparedness research sectors and are likely to continue to increase in sophistication throughout the foreseeable future. The essential quality of MANETs that make them well-suited for behavior therapies is their ability to support so-called ‘pervasive’ or ‘ubiquitous’ computing. Because the nodes of the network are free to move about in space, the individual will come into (and go out of) contact with various nodes of the network including human and automated sensors. The network is able to reassemble on-the-fly, thereby enabling behavior modification to travel with the individual undergoing therapy. This enables therapy to continue at home and school in a seamless fashion.
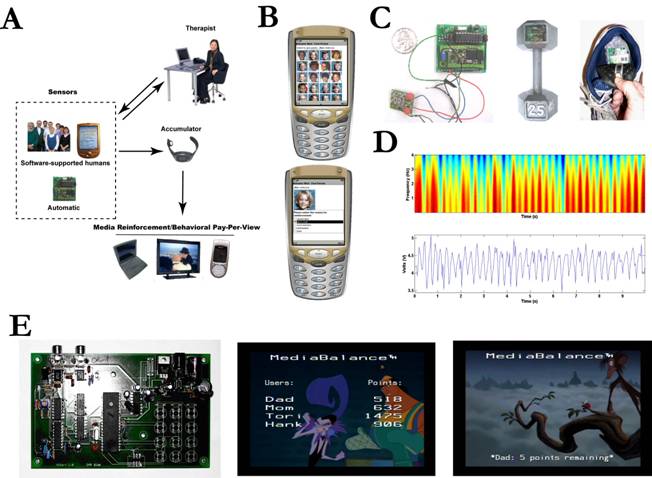
MediaBalance has developed wireless mobile ad hoc technology for improving (a) exercise behaviors in youth, (b) dietary behaviors in adolescents and adults, and (c) the treatment of the functional deficits associated with attention deficit hyperactivity disorder (ADHD) in home and classroom settings. The technology consists of networks of devices including hardware for embedded sensors, software to support humans in detecting behaviors, and software for managing behavior plans.
MediaBalance, Inc. was founded in 2003 by Dr. Alejandro Terrazas. The company’s mission is to bring high technology and behavioral psychology to bear on the nation’s most critical health problems. Dr. Terrazas has unique experience appropriate to this task. He has a Ph.D. in Psychology and extensive experience in object oriented programming, embedded systems, and database design. Dr. Terrazas completed a two-year fellowship at the National Institutes of Mental Health where he conducted human brain imaging experiments using virtual reality. He is the former Associate Director of the Machine Interface Network Design (MIND) Laboratory at Michigan State University where he oversaw R & D efforts in Internet controllable robotics, virtual reality, neuroinformatics, and human computer interaction. Dr. Terrazas is an authority on the Java computer programming language. In 2000, he was appointed to an elite industry and academic consortium that produced the Java Advanced Imaging Specification 1.1 (JSR 34). He is the author of the book Java Media API's: Cross-platform Imaging, Media, and Visualization (SAMS/Pearson Press, ISBN: 0-672-32094-0).
MediaBalance has developed an active research program based on using high technology for behavior treatments. Dr. Terrazas is currently the P.I. on three NIH-funded Phase I SBIR grants using his behavioral technology: (a) NIDDK 1 R43 DK070482-01 to modify physical activity behaviors in sedentary and obese youth (b) NIDDK 1 R43 DK075268-01 to modify weight loss and maintenance behaviors in adults, and (c) NIMH 1 R43 MH076359-01 to implement evidence-based behavioral therapies in children with attention deficit hyperactivity disorder.
Unfortunately, substantial impediments to widespread use of behavior therapy remain. Whereas the vast majority of children with ADHD receive pharmacotherapy at some point in their lives, only about 10% ever receive behavior therapy (Bosco & Robin, 1988). Common obstacles include noncompliance with or inconsistent implementation of behavior plans by parents and teachers, who view the demands of implementing the intervention as overly burdensome. Similarly, the systematic tracking and logging of data is a substantial problem for many individuals applying a behavior plan, yet, it is mandatory for the effective application of therapy. These difficulties are multiplied when more than one individual is undergoing behavior therapy in the same classroom or home environment and are further exacerbated when the therapies are individualized. There is a pressing need to overcome these barriers so that evidence-based behavioral treatments can be translated to the field, where they are badly needed.References:Bosco, J. & Robin, S. (1980). Hyperkenesis: Prevalence and treatment. In C. Whalen & B. Henker (Eds.) Hyperactive children: The social ecology of identification and treatment (pp. 173-187). New York, Academic Press.
Data from the NIMH collaborative Multimodal Treatment Study of Children with ADHD (MTA) suggests that the optimal treatment of the wide range of problems associated with ADHD, especially those extending beyond ADHD symptoms (e.g., oppositional/aggression behavior, parent-child conflict, academic problems), are best addressed by combining medication with behavioral interventions (MTA Cooperative Group, 1999). Project Co-Investigator Dr. Hoza has shown a dose-response relationship between the intensity of behavior therapy and improvements in functional deficits associated with ADHD—indeed, in some cases, increasing the intensity of behavior therapy can eliminate the need for pharmacotherapy (Hoza et al., 1992). Furthermore, use of behavior therapy concurrently with medication substantially reduces the required dosage of medication, presumably also reducing the associated risks of side effects (MTA Cooperative Group, 1999). The issue of side effects has received renewed attention given recent findings of constitutive changes in gene expression following administration of methylphenidate in rats (Chase et al., 2005).
Reference cited:
1.MTA Cooperative Group. (1999). 14-month randomized clinical trial of treatment strategies for attention deficit hyperactivity disorder. Arch Gen Psychiatry, 56:1073-1086.1.
2. Hoza, B. Pelham, W. E., Sams, S. E., & Carlson, C. (1992). An examination of the “dosage” effects of both behavior therapy and methylphenidate on the classroom performance of two ADHD children. Behav Modif, 16(2):164-92.
3.MTA Cooperative Group. (1999). Moderators and mediators of treatment response for children with attention-deficit/hyperactivity disorder: The multimodal treatment study of children with attention-deficit/hyperactivity disorder. Arch Gen Psychiatry, 56:1088-1096.
4. Chase, T. D., Carrey, N., Brown, R. E., & Wilkinson, M (2005) Methylphenidate differentially regulates c-fos and fosB expression in the developing rat striatum Brain Res Dev Brain Res, Jun 30;157(2):181-91.